



Gastroesophageal Reflux (GER) and Gastroesophageal Reflux Disease (GERD) in Adults
Gastroesophageal reflux (GER) occurs when stomach contents flow back up into the esophagus—the muscular tube that carries food and liquids from the mouth to the stomach.
GER is also called acid reflux or acid regurgitation because the stomach’s digestive juices contain acid. Sometimes people with GER can taste food or acidic fluid in the back of the mouth. Refluxed stomach acid that touches the lining of the esophagus can cause heartburn. Also called acid indigestion, heartburn is an uncomfortable, burning feeling in the midchest, behind the breastbone, or in the upper part of the abdomen—the area between the chest and the hips.
Occasional GER is common. People may be able to control GER by
- avoiding foods and beverages that contribute to heartburn, such as chocolate, coffee, peppermint, greasy or spicy foods, tomato products, and alcoholic beverages
- avoiding overeating
- quitting smoking
- losing weight if they are overweight
- not eating 2 to 3 hours before sleep
- taking over-the-counter medications.
What is GERD?
Gastroesophageal reflux disease (GERD) is a more serious, chronic––or long lasting––form of GER. GER that occurs more than twice a week for a few weeks could be GERD, which over time can lead to more serious health problems. People with suspected GERD should see a health care provider.
What causes GERD?
Gastroesophageal reflux disease results when the lower esophageal sphincter—the muscle that acts as a valve between the esophagus and stomach—becomes weak or relaxes when it should not, causing stomach contents to rise up into the esophagus.
Abnormalities in the body such as hiatal hernias may also cause GERD. Hiatal hernias occur when the upper part of the stomach moves up into the chest. The stomach can slip through an opening found in the diaphragm. The diaphragm is the muscle wall that separates the stomach from the chest. Hiatal hernias may cause GERD because of stomach acid flowing back up through the opening; however, most produce no symptoms.
Other factors that can contribute to GERD include
- obesity
- pregnancy
- certain medications, such as asthma medications, calcium channel blockers, and many antihistamines, pain killers, sedatives, and
- antidepressants
- smoking, or inhaling secondhand smoke
People of all ages can develop GERD, some for unknown reasons.
What is the gastrointestinal (GI) tract?
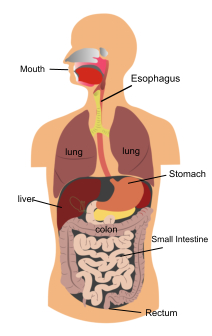
The GI tract is a series of hollow organs joined in a long, twisting tube from the mouth to the anus. The movement of muscles in the GI tract, along with the release of hormones and enzymes, starts the digestion of food. The upper GI tract includes the mouth, esophagus, stomach, small intestine, and duodenum, which is the first part of the small intestine.
GERD results when the lower esophageal sphincter—the muscle that acts as a valve between the esophagus and stomach—becomes weak or relaxes when it should not, causing stomach contents to rise up into the esophagus.
What are the symptoms of GERD?
The main symptom of GERD is frequent heartburn, though some adults with GERD do not have heartburn. Other common GERD symptoms include
- a dry, chronic cough
- wheezing
- asthma and recurrent pneumonia
- nausea
- vomiting
- a sore throat, hoarseness, or laryngitis—swelling and irritation of the voice box
- difficulty swallowing or painful swallowing
- pain in the chest or the upper part of the abdomen
- dental erosion and bad breath
How is GERD treated?
Treatment for GERD may involve one or more of the following, depending on the severity of symptoms: lifestyle changes, medications, or surgery.
Lifestyle Changes
Some people can reduce GERD symptoms by
- losing weight, if needed
- wearing loose-fitting clothing around the stomach area, as tight clothing can constrict the area and increase reflux
- remaining upright for 3 hours after meals
- raising the head of the bed 6 to 8 inches by securing wood blocks under the bedposts––just using extra pillows will not help
- avoiding smoking and being around others who are smoking
Medications
People can purchase many GERD medications without a prescription; however, people with persistent symptoms should still see a health care provider.
Antacids, which include over-the-counter medications such as Alka-Seltzer, Maalox, Mylanta, Rolaids, and Riopan, are a first-line approach health care providers usually recommend to relieve heartburn and other mild GERD symptoms. Antacids, however, can have side effects, including diarrhea and constipation.
H2 blockers, such as cimetidine (Tagamet HB), famotidine (Pepcid AC), nizatidine (Axid AR), and ranitidine (Zantac 75), decrease acid production. These medications are available in both over-the-counter and prescription strengths. H2 blockers provide short-term or on-demand relief and are effective for many people with GERD symptoms. They can also help heal the esophagus, although not as well as proton pump inhibitors (PPIs).
PPIs include omeprazole (Prilosec, Zegerid), lansoprazole (Prevacid), pantoprazole (Protonix), rabeprazole (Aciphex), and esomeprazole (Nexium), which are available by prescription. Omeprazole and lansoprazole also come in over-the-counter strength. PPIs are more effective than H2 blockers and can relieve symptoms and heal the esophageal lining in most people with GERD. Health care providers most commonly prescribe PPIs for long-term management of GERD. However, studies show people who take PPIs long term or in high doses are more likely to have hip, wrist, and spinal fractures. People should take these medications on an empty stomach in order for stomach acid to activate them.
Prokinetics, which include bethanechol (Urecholine) and metoclopramide (Reglan), help make the stomach empty faster. However, both bethanechol and metoclopramide have side effects that often limit their use, including nausea, diarrhea, tiredness, depression, anxiety, and problems with physical movement. Prokinetics can interact with other medications, so people taking prokinetic agents should tell their health care provider about all medications they are taking.
Antibiotics, including one called erythromycin, have been shown to improve gastric emptying. Erythromycin has fewer side effects than bethanechol and metoclopramide; however, like all antibiotics, it can cause diarrhea.
All of these medications work in different ways, so combinations of medications may help control symptoms. People who get heartburn after eating may take antacids and H2 blockers. The antacids neutralize stomach acid, and the H2 blockers stop acid production. By the time the antacids stop working, the H2 blockers have stopped acid production.
Surgery
When a person cannot manage severe GERD symptoms through medication or lifestyle changes, a health care provider may recommend surgery. A health care provider may also recommend surgery for GERD that results from a physical abnormality or for GERD symptoms that lead to severe respiratory problems. Fundoplication is the standard surgical treatment for GERD and leads to long-term reflux control in most cases. A gastroenterologist or surgeon may also use endoscopic techniques to treat GERD. However, the success rates of endoscopic techniques are not completely known, as researchers have not tested them enough in clinical trials. People are more likely to develop complications from surgery than from medications. Anti-reflux surgery is most successful in people younger than 50.
Fundoplication is an operation to sew the top of the stomach around the esophagus to add pressure to the lower end of the esophagus and reduce reflux. A surgeon performs fundoplication using a laparoscope, a thin tube with a tiny video camera attached used to look inside the body. The surgeon performs the operation at a hospital or an outpatient center, and the person receives general anesthesia. People can leave the hospital or outpatient center in 1 to 3 days and return to their daily activities in 2 to 3 weeks.
Endoscopic techniques, such as endoscopic sewing and radiofrequency, help control GERD in a small number of people. Endoscopic sewing uses small stitches to tighten the sphincter muscle. Radiofrequency creates heat lesions that help tighten the sphincter muscle. Surgery for both techniques requires an endoscope. A surgeon performs the operation at a hospital or an outpatient center, and the person receives anesthesia. Although the devices for these procedures are approved, results may not be as good as laparoscopic surgery, and these procedures are not commonly used.
If you have any questions or wish to schedule an appointment, please do not hesitate to call the office at (706) 548-0058. Remember that we usually require that you see a primary care physician (your family doctor or PCP) before we can schedule you. If you are having a medical emergency, get medical attention immediately at your nearest healthcare provider:
Athens Regional Medical Center: (706) 475-7000
St. Mary's Hospital: (706) 354-3000
This informational material is taken from the National Digestive Diseases Information Clearinghouse, a division of the U.S. Department of Health and Human Resources.
Please see the Contact Us page for street maps.
Click here to
Request an Appointment.