




Constipation
 The lower GI tract
The lower GI tractConstipation is a condition in which a person has fewer than three bowel movements a week or has bowel movements with stools that are hard, dry, and small, making them painful or difficult to pass. People may feel bloated or have pain in their abdomen—the area between the chest and hips. Some people think they are constipated if they do not have a bowel movement every day. Bowel movements may occur three times a day or three times a week, depending on the person.
Most people get constipated at some point in their lives. Constipation can be acute, which means sudden and lasting a short time, or chronic, which means lasting a long time, even years. Most constipation is acute and not dangerous. Understanding the causes, prevention, and treatment of constipation can help many people take steps to find relief.
What is the gastrointestinal (GI) tract?
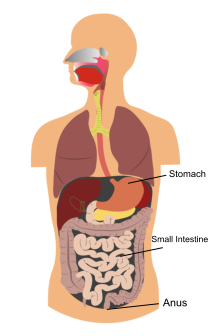
The GI tract is a series of hollow organs joined in a long, twisting tube from the mouth to the anus. The body digests food using the movement of muscles in the GI tract, along with the release of hormones and enzymes. Organs that make up the GI tract are the mouth, esophagus, stomach, small intestine, large intestine—which includes the appendix, cecum, colon, and rectum—and anus. The intestines are sometimes called the bowel. The last part of the GI tract—called the lower GI tract—consists of the large intestine and anus.
The large intestine absorbs water and any remaining nutrients from partially digested food passed from the small intestine. The large intestine then changes waste from liquid to a solid matter called stool. Stool passes from the colon to the rectum. The rectum is located between the last part of the colon—called the sigmoid colon—and the anus. The rectum stores stool prior to a bowel movement. During a bowel movement, stool moves from the rectum to the anus, the opening through which stool leaves the body.
What causes constipation?
Constipation is caused by stool spending too much time in the colon. The colon absorbs too much water from the stool, making it hard and dry. Hard, dry stool is more difficult for the muscles of the rectum to push out of the body.
Common factors or disorders that lead to constipation are
- diets low in fiber
- lack of physical activity
- medications
- life changes or daily routine changes
- ignoring the urge to have a bowel movement
- neurological and metabolic disorders
- GI tract problems
- functional GI disorders
Diets Low in Fiber
The most common cause of constipation is a diet with too little fiber. Fiber is a substance in foods that comes from plants. Fiber helps stool stay soft so it moves smoothly through the colon. Liquids such as water and juice help fiber to be more effective.
Older adults commonly do not get enough fiber in their diets. They may lose interest in eating because food does not taste the same as it once did, they do not feel hungry as often, they do not want to cook, or they have problems with chewing or swallowing. These factors may lead an older adult to choose foods that are quick to make or buy, such as fast foods or prepared foods, which are often low in fiber.
Lack of Physical Activity
A lack of physical activity can lead to constipation, although scientists do not know why. For example, constipation often occurs after an accident or during an illness when a person must stay in bed and cannot exercise. Lack of physical activity is thought to be one of the reasons constipation is common in older adults.
Medications
Medications that can cause constipation include
- pain medications, especially narcotics
- antacids that contain aluminum and calcium
- calcium channel blockers, which are used to treat high blood pressure and heart disease
- medications that treat Parkinson’s disease—a disorder that affects nerve cells in a part of the brain that controls muscle movement—because these medications also affect the nerves in the colon wall
- antispasmodics—medications that prevent sudden muscle contractions
- some antidepressants
- iron supplements
- diuretics—medications that help the kidneys remove fluid from the blood
- anticonvulsants—medications that decrease abnormal electrical activity in the brain to prevent seizures
Constipation can also be caused by overuse of over-the-counter laxatives. A laxative is medication that loosens stool and increases bowel movements. Although people may feel relief when they use laxatives, they usually must increase the dose over time because the body grows reliant on laxatives to have a bowel movement. Overuse of laxatives can decrease the colon’s natural ability to contract and make constipation worse. Continued overuse of laxatives can damage nerves, muscles, and tissues in the large intestine.
Life Changes or Daily Routine Changes
During pregnancy, women may be constipated because of hormonal changes or because the uterus compresses the intestine. Aging can affect bowel regularity, because of a gradual loss of nerves stimulating the muscles in the colon, which results in less intestinal activity. People can also become constipated while traveling, because their normal diet and daily routine are disrupted.
Ignoring the Urge to Have a Bowel Movement
People who ignore the urge to have a bowel movement may eventually stop feeling the need to have one, which can lead to constipation. Some people delay having a bowel movement because they do not want to use toilets outside their home, particularly public restrooms, or they feel they are too busy.
Neurological and Metabolic Disorders
Certain neurological and metabolic disorders can cause food to pass through the digestive system too slowly, leading to constipation. Neurological disorders, such as spinal cord injury and parkinsonism, affect the brain and spine. Parkinsonism is any condition that leads to the types of movement changes seen in Parkinson’s disease. Metabolic disorders, such as diabetes and hypothyroidism, disrupt the process the body uses to get energy from food. Hypothyroidism is a disorder that causes the body to produce too little thyroid hormone, which can cause many of the body’s functions to slow down.
GI Tract Problems
Some problems in the GI tract can compress or narrow the colon and rectum, causing constipation. These problems include
- adhesions—bands of tissue that can connect the loops of the intestines to each other, which may block food or stool from moving through the GI tract
- diverticulosis—a condition that occurs when small pouches, or sacs, form and push outward through weak spots in the colon wall; the pouches are called diverticula
- colon polyps—growths on the surface of the colon that can be raised or flat
- tumors—abnormal masses of tissue that result when cells divide more than they should or do not die when they should
- celiac disease—an immune reaction to gluten, a protein found in wheat, rye, and barley, that causes damage to the lining of the small intestine and prevents absorption of nutrients
Read more about the Celiac Disease Awareness Campaign at www.celiac.nih.gov.
Functional GI Disorders
Functional GI disorders are problems caused by changes in how the GI tract works. People with a functional GI disorder have frequent symptoms; however, the GI tract does not become damaged. Functional constipation often results from problems with muscle activity in the colon or anus that delay stool movement.
Functional constipation is diagnosed in people who have had symptoms for at least 6 months and meet the following criteria for the last 3 months before diagnosis:3
- Two or more of the following symptoms:
- straining to have a bowel movement at least 25 percent of the time
- having lumpy or hard stools at least 25 percent of the time
- feeling as though stool is still in the rectum after a bowel movement at least 25 percent of the time
- feeling as though something is blocking stool from passing at least 25 percent of the time
- using their fingers to help with stool passage at least 25 percent of the time
- having fewer than three bowel movements per week
- Rarely passing loose stools without the use of laxatives
- Not having irritable bowel syndrome (IBS)
IBS is a functional GI disorder with symptoms that include abdominal pain or discomfort, often reported as cramping, along with diarrhea, constipation, or both. Read more in Irritable Bowel Syndrome at www.digestive.niddk.nih.gov.
3- Longstreth GF, Thompson WG, Chey WD, et al. Functional bowel disorders. In: Drossman DA, ed. Rome III: The Functional Gastrointestinal Disorders. 3rd ed. Lawrence, KS: Allen Press, Inc.; 2006: 515–523.
How is constipation treated?
Treatment for constipation depends on the cause, severity, and duration of the constipation and may include one or more of the following:
- changes in eating, diet, and nutrition
- exercise and lifestyle changes
- medication
- surgery
- biofeedback
First-line treatments for constipation include changes in eating, diet, and nutrition; exercise and lifestyle changes; and laxatives. People who do not respond to these first-line treatments should talk with their health care provider about other treatments.
Eating, Diet, and Nutrition
The Academy of Nutrition and Dietetics recommends consuming 20 to 35 grams of fiber a day for adults. Americans consume only 15 grams a day on average.4 People often eat too many refined and processed foods from which the natural fiber has been removed. A health care provider can help plan a diet with the appropriate amount of fiber. A list of high-fiber foods is shown below. People prone to constipation should limit foods that have little or no fiber, such as ice cream, cheese, meat, and processed foods.
4- Slavin JL. Position of the American Dietetic Association: health implications of dietary fiber. Journal of the American Dietetic Association. 2008;108:1716–1731.
Examples of Foods That Have Fiber |
|
| Beans, cereals, and breads | Fiber |
| ½ cup of beans (navy, pinto, kidney, etc.), cooked | 6.2–9.6 grams |
| ½ cup of shredded wheat, ready-to-eat cereal | 2.7–3.8 grams |
| ⅓ cup of 100% bran, ready-to-eat cereal | 9.1 grams |
| 1 small oat bran muffin | 3.0 grams |
| 1 whole-wheat English muffin | 4.4 grams |
| Fruits | |
| 1 small apple, with skin | 3.6 grams |
| 1 medium pear, with skin | 5.5 grams |
| ½ cup of raspberries | 4.0 grams |
| ½ cup of stewed prunes | 3.8 grams |
| Vegetables | |
| ½ cup of winter squash, cooked | 2.9 grams |
| 1 medium sweet potato, baked in skin | 3.8 grams |
| ½ cup of green peas, cooked | 3.5–4.4 grams |
| 1 small potato, baked, with skin | 3.0 grams |
| ½ cup of mixed vegetables, cooked | 4.0 grams |
| ½ cup of broccoli, cooked | 2.6–2.8 grams |
| ½ cup of greens (spinach, collards, turnip greens), cooked | 2.5–3.5 grams |
Source: U.S. Department of Agriculture and U.S. Department of Health and Human Services, Dietary Guidelines for Americans, 2010
Drinking water and other liquids, such as fruit and vegetable juices and clear soups, may make fiber in the diet more effective in normalizing bowel function and maintaining regularity. A health care provider can give advice about how much a person should drink each day based on the person’s health and activity level and where the person lives.
Exercise and Lifestyle Changes
Engaging in daily exercise can help people with constipation. Another strategy is to try to have a bowel movement at the same time each day. The best time is 15 to 45 minutes after breakfast because eating helps stimulate the colon. People with constipation should reserve enough time to have a bowel movement and be sure not to ignore the urge to have a bowel movement.
Medication
When a medication is causing constipation, the health care provider may suggest the person stop taking the medication or switch to a different medication.
Laxative medications and enemas may be recommended for people who have made diet and lifestyle changes and are still constipated. Laxatives taken by mouth are available in liquid, tablet, powder, and granule forms.
- Bulk-forming agents. Brand names include Metamucil, FiberCon, Citrucel, Konsyl, and Serutan. Bulk-forming agents absorb fluid in the intestines, making stools bulkier, which helps trigger the bowel to contract and push stool out. These supplements should be taken with water or they can cause obstruction. Bulk-forming agents are generally considered the safest laxative, but they can interfere with the absorption of some medications. Many people also report no relief after taking bulk-forming agents and suffer from bloating and abdominal pain.
- Osmotic agents. Brand names include Milk of Magnesia, Fleet Phospho-Soda, Cephulac, Sorbitol, and Miralax. Osmotic agents help stool retain fluid, increasing the number of bowel movements and softening the stool. These laxatives are usually used by people who are bedridden or cannot take bulk-forming agents. Older adults and people with heart or kidney failure should be careful when taking osmotic agents because they can cause dehydration or a mineral imbalance.
- Stool softeners. Brand names include Colace, Docusate, and Surfak. Stool softeners help mix fluid into stools to soften them. Stool softeners may be suggested for people who should avoid straining in order to pass a bowel movement; they are often recommended after childbirth or surgery.
- Lubricants. Brand names include Fleet and Zymenol. Lubricants work by coating the surface of stool, which helps the stool hold in fluid and pass more easily. Lubricants are simple, inexpensive laxatives that may be recommended for people with anorectal blockage.
Other types of laxatives include
- Stimulants. Brand names include Correctol, Dulcolax, Purge, and Senokot. Stimulant laxatives cause the intestines to contract, which moves stool. Stimulants should be reserved for constipation that is severe or has not responded to other treatments. People should not use stimulant laxatives containing phenolphthalein, as phenolphthalein may increase the likelihood of cancer. Most laxatives sold in the United States do not contain phenolphthalein.
- Chloride channel activators. Lubiprostone (Amitiza) is a chloride channel activator available with a prescription. This type of laxative increases fluid in the GI tract. Lubiprostone has been shown to be safe when used for 6 to 12 months.
People who depend on laxatives to have a bowel movement need to talk with their health care provider about how to slowly stop using them. For most people, stopping laxatives restores the colon’s natural ability to contract.
Surgery
Surgery may be needed to correct an anorectal blockage caused by rectal prolapse. Surgical removal of the colon may be an option for people whose colon muscles do not work properly, causing severe symptoms that do not respond to treatment. However, the benefits of this surgery should be weighed against possible complications, which include abdominal pain and diarrhea.
Biofeedback
People with chronic constipation caused by problems with the anorectal muscles can use biofeedback to retrain the muscles. Biofeedback uses special sensors to measure bodily functions. The measurements are displayed on a video screen as line graphs and sounds indicate when the person is using the correct muscles. The health care provider uses the information to help the person modify or change abnormal function. The person practices at home. The person may need to continue practicing for 3 months to get the most benefit from the training.
If you have any questions or wish to schedule an appointment, please do not hesitate to call the office at (706) 548-0058. Remember that we usually require that you see a primary care physician (your family doctor or PCP) before we can schedule you. If you are having a medical emergency, get medical attention immediately at your nearest healthcare provider:
Athens Regional Medical Center: (706) 475-7000
St. Mary's Hospital: (706) 354-3000
This informational material is taken from the National Digestive Diseases Information Clearinghouse, a division of the U.S. Department of Health and Human Resources.
Please see the Contact Us page for street maps.
Click here to
Request an Appointment.